Exactly. And I insist that by exhaling, you will reduce neither the PpCO2 nor the CO2 in the blood. The alveolar PpCO2 will remain identical to the level prior the exhale, because the transpulmonary pressure difference between full and empty lungs is several orders lower than the ambient pressure and hence has no meaningfull impact. So no change in alveolar PpCO2 due to the exhale. And since the lung volume is reduced after the exhale, the PaCO2/PACO2 (arterial/alveolar) diffusion will equalize quicker with less volume of CO2 extracted from the blood. That means then, that in fact by exhaling you may increase your arterial PpCO2, not reducing it, gaining so more tolerance against hypoxia.
There are two things here which we must separate: 1. does ascending per se lower hypoxia tolerance? and, 2. does exhaling counteract this effect, thereby maintaining or even enhancing hypoxia tolerance?
In the first instance:
The data from Líner et al (1993) clearly demonstrates that PACO2 decreases during ascent. Presuming there is rapid equalization between PACO2 and paCO2, as you suggest, this would point to a reduction in PaCO2 also. Further, their data clearly demonstrates that a large quantity of CO2 is mobilized into the lungs upon decompression. This CO2 coming out of the blood. The additional graphs the offer, on gas exchange, further demonstrates this very well, and I quote from this reference:
"...during the ascent, the PACO2 decreased,..."
"...after leaving the bottom, CO2 moved into the alveoli at an [
accelerating ] rate reaching 218 +/- 13 ml/m/m2 ... late in the ascent."
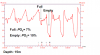
You can see this also from Lanphier & Rahn (1963) article: CO2 moves back into the lungs and PACO2 drops. Fig.7 clearly shows PaCO2 dropping.
"...PCO2....decreases rather abruptly on ascent."
"The volume of CO2 is low at the outset .... until the beginning of ascent, when a relatively large increase occurs."
"... unexpectedly low values of PCO2 found upon surfacing from dives."
"The volume of CO2 transferred to the lungs ...... modifies the fall in PCO2 to a considerable extent."
And, elsewhere, in Hong et al. (1963):
"Upon return to the surface CO2 leaves the blood...". Fig. 7 of this publication clearly shows movement of CO2 out of the blood and into the lungs and this processing accelerating with the rate of decompression, i.e., with decreasing depth. The only thing the dropping pCO2 does is offer subjective/relative relief in the urge to breathe, not enhanced hypoxic tolerance. Indeed, hypoxia tolerance would decrease
In the second instance: it sounds plausible, but let's measure it!
I propose that someone with a flow-though CO2 gas analyzer do the following very simple test: breath-hold at TLC until contractions start, after which you exhale progressively, measuring pACO2 continuously as you exhale to FRC